

PrEP (Pre-Exposure Prophylaxis)
While PrEP is highly effective at preventing HIV infection and has been available for more than 10 years, many people who might benefit from taking it have not received a prescription. A lack of provider knowledge about PrEP - both PCP and GI, discomfort discussing sexual behavior, patients’ negative perceptions of PrEP, financial and staffing limitations, medical mistrust, and low health literacy all impede PrEP access. Currently, there are no explicit interactions or negative indications between many available IBD therapeutic (biologic, small molecule, etc) and PrEP, but there are some things to look out for and things that may make your bloodwork funky if you take certain medications (SCROLL TO THE BOTTOM! for more info!)
TLDR: the benefits of having STI protection (whether that is through PrEP in things like Truvada or PEP like DoxyPEP) probably outweigh the cons of not having protection.
PrEP
(short for Pre-Exposure Prophylaxis)
Also see info on this page about IBD and PrEP. See this page for IBS Medications and PrEP.
PrEP (pre-exposure prophylaxis) is an FDA-approved, CDC recommended daily prevention pill prescribed to people of all genders, transgender and gender diverse experience, races, ethnicities, and ages who do not have HIV but who are vulnerable to getting HIV.
HIV does not only/exclusively affect the LGBTQ+ community, but it has and continues to affect queer and trans people disproportionately - due to a combination of factors including lack of access to care, socioeconomic disparity, and more.
And, unlike so many IBD medications on the first prior authorization, PrEP is FULLY APPROVED BY INSURANCE!
As of July 2021, almost all insurance plans and state Medicaid programs must cover the cost of PrEP as well as the required clinic visits and lab tests, with no cost sharing—this means the entire experience of maintaining a prescription to PrEP should now be totally free for almost all insured individuals. (hopefully it stays that way)
It can either be a pill that you take every day or an injection that you get every two months.
Taken daily, PrEP is up to 99% effective at preventing new HIV infections. Many people who take PrEP report feeling a sense of peace of mind while having sex, because they are taking their health into their own hands. That peace of mind reduces the fear and stigma associated with HIV.
How does PrEP work?
PrEP is prescribed as a preventative strategy, meaning people take the anti-HIV drug to lower their chances of contracting when they encounter it through sex or drug use.
With PrEP, if you do get exposed to HIV, the medicine can stop HIV from entering cells in your body by blocking the enzyme it needs to reproduce, so you don’t get sick.
PrEP is very effective when you take it consistently.
A multi-center retrospective cohort study with 195 patients with IBD (65 of them people living with HIV and IBD) showed there were no significant differences in terms of hospitalization, surgery or intestinal complications (strictures, fistulas, abscesses) in people living with HIV and IBD vs. people with IBD without HIV.
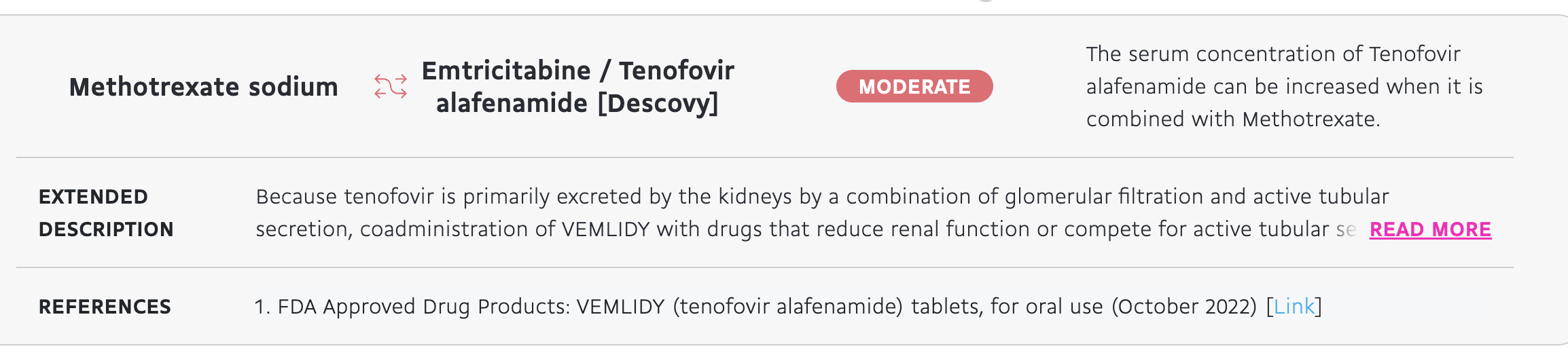
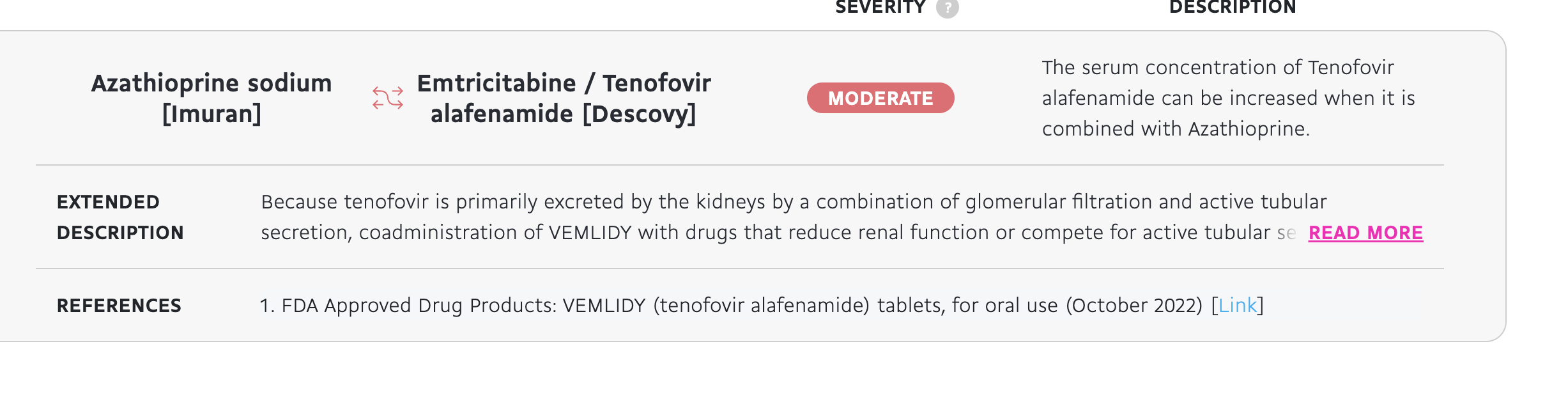
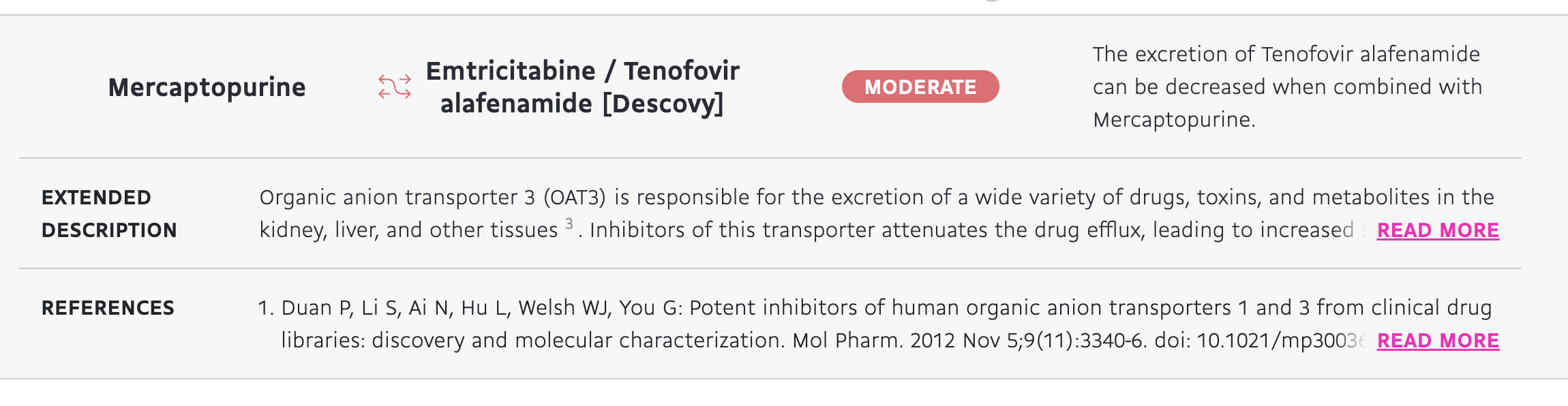
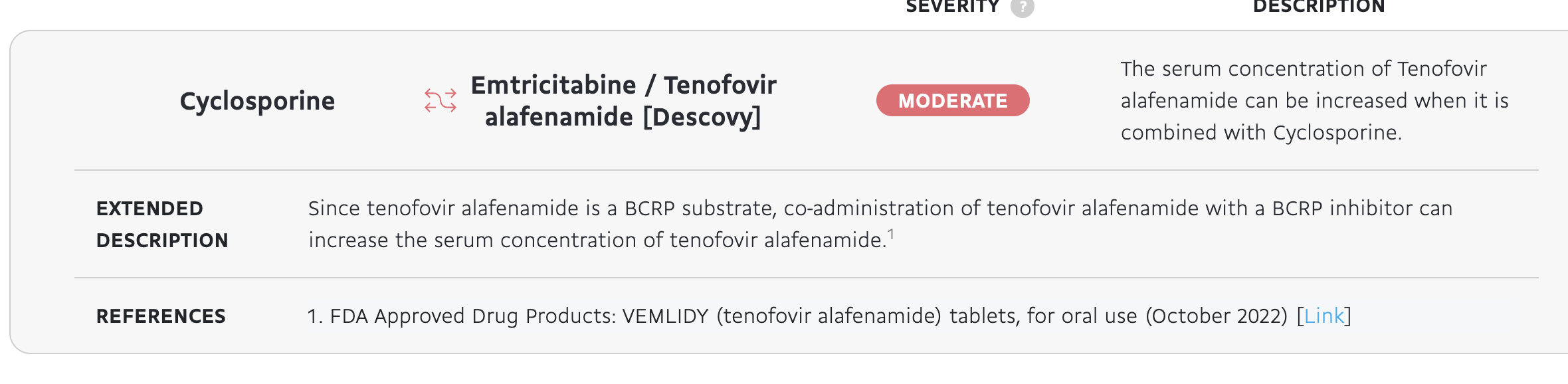
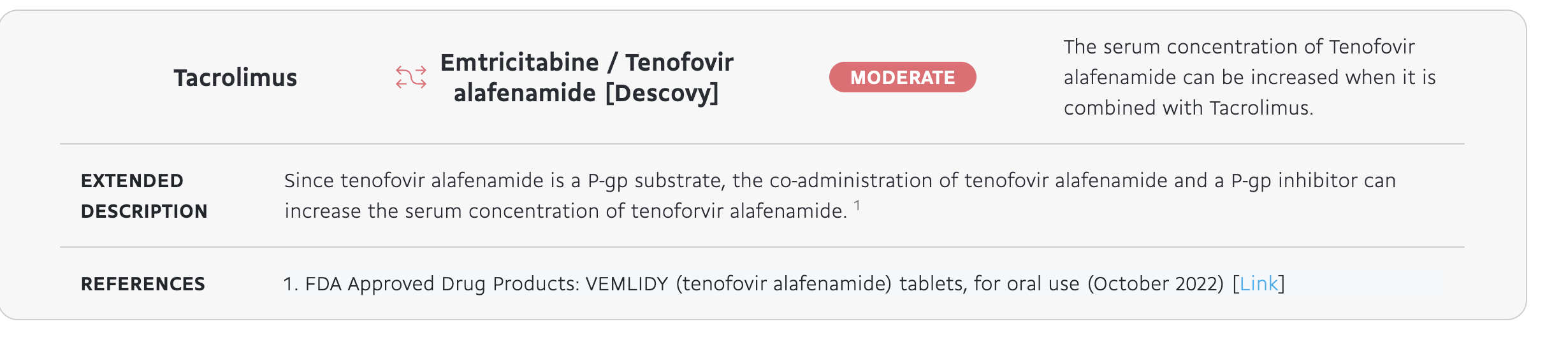
When cross checking interactions between PrEP and IBD medications, including biologics, small molecules, interactions were NOT found between biologics and small molecules such as Stelara and Zeposia, but a moderate interaction was found between Descovy and Mesalamine (Asacol, etc) and Prednisone and Immunomodulator thiopurine medications Methotrexate, Mercaptopurine (6-MP) Azathiopurine (Imuran), and cyclosporine.
However, for Thiopurines increase the serum concentration of Descovy because of how the drug is metabolized - so this may mean you just have to go on a lower dose perhaps. This is a discussion for you and your doctor.
Mesalamine is a touch different, and if you have a history of kidney disease or kidney injury, speak to your doctor.
A moderate interaction was found between Infliximab (remicade) and Humira (Adalimumab) and Descovy - this is similar to the interaction between Thiopurines, where the metabolism of Remicade/Humira just increases. (The metabolism of Tenofovir alafenamide (Descoy) can be increased when combined with Infliximab due to CYP450 enzyme metabolism)
See below for further expansion on interactions and references. I did this for every prescribed IBD drug I could find. Obviously check with your doctor.
Some people with IBD may need a little extra blood work than people without IBD before starting PrEP to make sure your liver and kidneys are all good to go.
For the vast majority of people, it is just fine (even if there is a lot going on/comorbidities - I have a heart condition and IBD and everything was fine for me).
For example, if you have a comorbid liver condition or extraintestinal manifestation (EIM) like primary sclerosing cholangitis (PSC), it is important to talk to your gastroenterology and hepatology care team and discuss wanting to start PrEP.
This doesn't mean that if you have a liver condition or history of elevated or abnormal liver enzymes you should never talk to your doctor about PrEP - it is just very important to monitor these things so your liver stays strong and healthy!
PrEP is overall a very effective and safe medicine, it is just important to make sure it is safe for you too!
What kinds of PrEP are there and how do I get it?
Truvada and Descovy are the only two brand-name PrEP medications approved for PrEP use by the FDA and CDC.
A generic equivalent to Truvada has also been approved for use in the US (generic tenofovir/emtricitabine)
Truvada can be prescribed for adults and adolescents, and Descovy can be prescribed to adults and adolescents (excluding those who have receptive vaginal sex) - talk to your doctor though, because as we know in IBD, things are prescribed “off-label” or for a use other than their ‘original’ use all of the time!
For anyone interested in PrEP, there’s a handful of resources, like PrEP Locator and Greater Than Aids, that can help you find a PrEP provider near you.
Your local health department and your doctor’s office if you are comfortable talking to your PCP or other HCP about it may be able to write you a prescription.
Once you have your prescription, it’s important to know that PrEP may only be available at certain pharmacies. Be sure to verify pharmacy information with your provider during your appointment! (for example, CVS may carry it, but a local independent pharmacy may not.)
If you’re concerned about having conversations about PrEP, it’s best to plan ahead to make those conversations successful.
Make sure your provider is knowledgeable about PrEP and is comfortable with prescribing it.
Calling your provider’s office/clinic in advance is a great way to make sure this is a service they can provide.
Once you’re at your appointment, be prepared to share that you’d like to start PrEP.
You can also say that you’re looking to take preventative medication to avoid contracting HIV, or refer to PrEP’s brand names (Truvada or Descovy) to introduce the topic of PrEP.
Your provider will likely ask some questions about your sexual activity and drug use, which is part of their process to determine how you will benefit from being on PrEP (and get insurance approval. This is also a great opportunity to ask questions you have about PrEP.
Last, if your provider is not comfortable prescribing PrEP and providing the necessary related care (like ordering quarterly labs), there are specialty clinics that can provide it.
You should never be discriminated against or shamed for taking care of your sexual health, and there are providers who will prescribe you preventative medication, it’s just a matter of finding them!
If talking in person (IRL, face to face, etc) isn’t comfortable - and that’s understandable - you can try sending a portal message (for example, 99% of healthcare systems and clinics have some sort of messaging like Epic/MyChart or an app where you can communicate with your clinic.) This is a place where you can send a message that you are interested in an appointment discussing PrEP.
It is very important to stay on top of infection prevention measures when having IBD, especially on immunomodulators or steroids and things like PrEP are a great way to do that. (and get your flu shot, COVID vaccine, etc)
Things like DoxyPEP and PrEP are overall a good idea to consider - it’s better to have prevention against STIs and the small risk of side effects from antibiotics (tummy upset, etc) than the bigger negative consequences that can come from untreated STIs, especially when living with IBD.Everyone is different, but if you are someone in that situation, the benefits may outweigh the potential risks and hopefully there is more information and research available soon on best options for people like us.
Every provider and person is different, so some may have you schedule an appointment after that, and some may do a telephone visit, and some may do something different. It just depends on your doctor and your situation, but this may be an easier way to start the conversation.
If you have a liver condition or something going on there, things are different and should talk to your doctor, but for the most part, the consensus is not having gonorrhea, syphilis and chlamydia or HIV is better than having those infections, especially with the IBD and everything.
Of course, I am not your doctor, and this is something that will vary from person to person, but DoxyPEP/PEP/PrEP are are examples of risk-benefit analysis you need to weigh, and for a lot of people, the benefits outweigh the risks. All of life is risk-benefit and impact calculus, and medicine is no different.You may consider PrEP if:
PrEP is prescribed to adults without HIV and adolescents who have anal and/or vaginal sex and are at a higher risk of contracting HIV.
PrEP is also prescribed to people who share syringes and needles for drug use with someone who is living with HIV.
However, is not just for cisgender gay men and people who use intravenous drugs.
HIV can affect anyone, regardless of their sexual orientation, gender, transgender experience, race, ethnicity, or age.
You may consider PrEP if:
You have more than one sex partner.
You don’t always use condoms (external or internal) when having vaginal or anal intercourse.
You are in an ongoing relationship with someone who has HIV.
You are unsure of your partner’s HIV status.
You have been diagnosed with an STD/STI in the past six months.
You have injected drugs in the past six months and have shared needles.
Do not consistently use condoms
Engage in sex with multiple or anonymous partners
Have repeatedly taken PEP (post-exposure prophylaxis) or on-demand PrEP
Are considering pregnancy and have a partner living with HIV
DoxyPEP
DoxyPEP means taking the antibiotic doxycycline after sex to prevent getting certain sexually transmitted infections (STIs).
It is like a morning-after pill but for STIs - DoxyPEP is generally well-tolerated and can reduce the likelihood of getting a bacterial STI, t
Taking DoxyPEP lowers your chance of getting syphilis, gonorrhea, and chlamydia by about two-thirds.
DoxyPEP might be for you if you are an adult gay man, transgender man, bisexual individual and other men who have sex with men, or a transgender woman at increased risk for STIs.
If you are living with HIV or are taking HIV pre-exposure prophylaxis (PrEP) and/or have had a bacterial STI in the past year (syphilis, chlamydia, gonorrhea), DoxyPEP might be a good idea to bring up with your healthcare provider too.
NOTE: if taking doxy (or minocycline)
Take doxyPEP with at least 8 ounces of water and food. This can help reduce side effects like nausea, upset stomach, and esophageal irritation
Do not lie down for one hour after taking doxycycline - the pill can irritate or burn your esophagus
Do not take doxycycline within two hours of having any dairy products, antacids and supplements with iron, calcium, or magnesium (reduces absorption)
Wear sunscreen or cover up to stay protected from the sun while taking doxycycline (makes you more susceptible to sunburn)
Interactions
Thiopurines/Immunomodulators and Potential Interactions
Applies to all thiopurines (may be prescribed a different flavor (6-MP, Imuran, Tacrolimus, Cyclosporine, or Methotrexate)
The serum concentration (aka, how much of the medicine is in your blood/blood concentration of the drug) may be increased when you are taking both of these medications because of how both medicines are metabolized (kidney stuff).
Mesalamine (Canasa, Pentasa, Asacol, Lialda)
This applies to all flavors of mesalamine you may be prescribed (it’s all the same chemically, just under a different brand - Asacol, Pentasa, Lialda, etc)
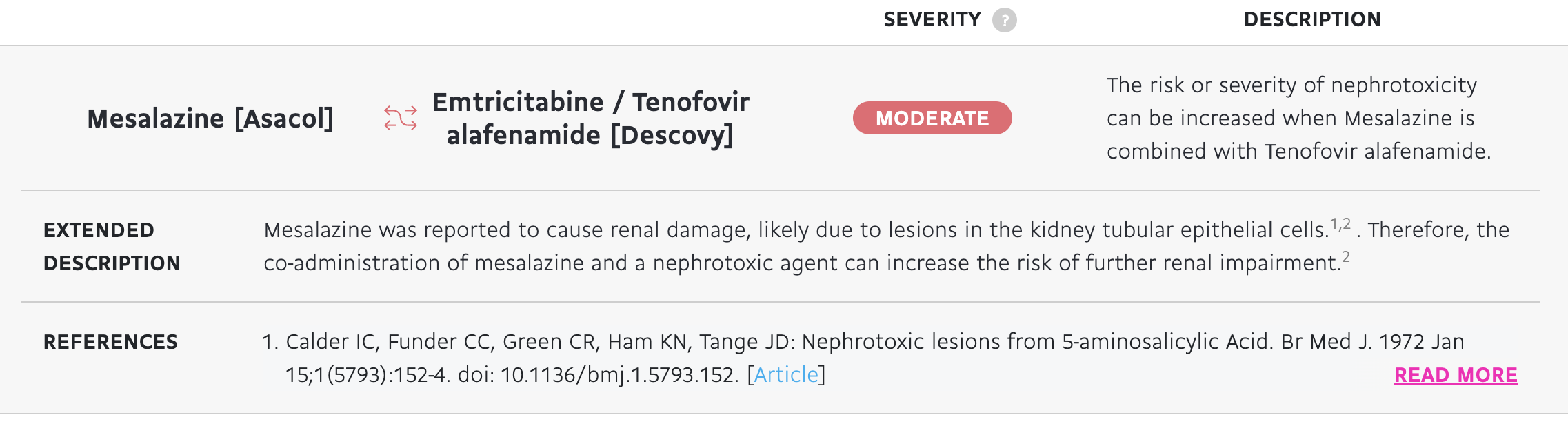
When mesalamine is combined with Descovy, risk for kidney lesions or nephrotoxicity is increased.
This may be increased if you have a previous history of kidney injury or disease (previous lesions in the kidney tubular epithelial cells), but regardless, be cautious abbout combining mesalamine and descovy as it can lead to nephrotoxicity (kidney injury).
5-ASAs are already nephrotoxic, so if you have a kidney disease, your doctor probably won’t have you on it or combine these anyway.
But ask your doctor! This is not a GUARANTEE, just a risk!
Biologics and Biosimilars (So Many To Include Here, Working On That)

We love biologics! No explicit interactions! (and everything else is cool too) (but Stelara treated me well)
Remicade (Infliximab) and Humira (Adalimumab) and Cimizia (Certolizumab pegol)
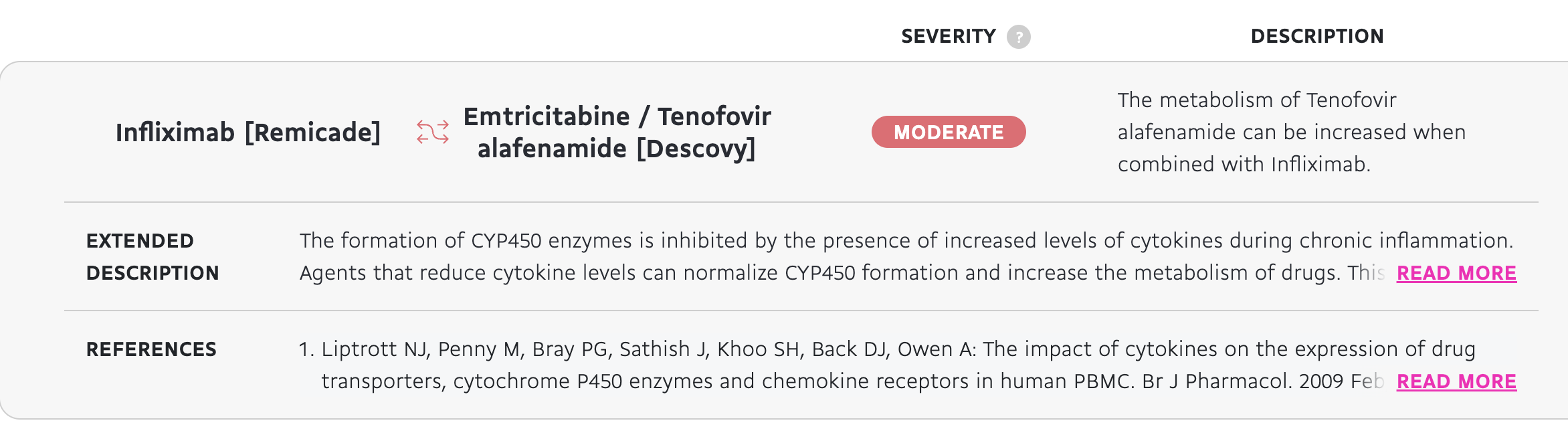
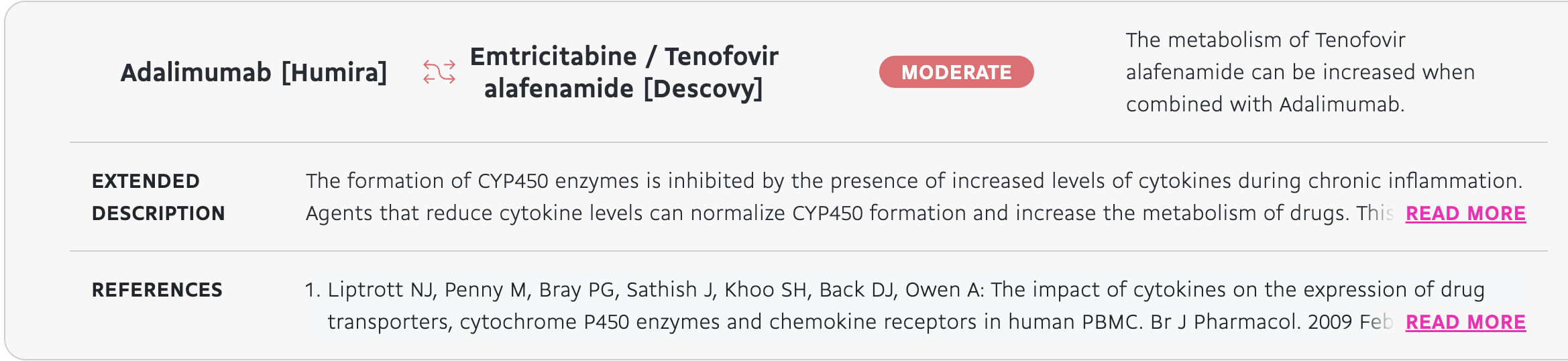

There is an enzyme in your liver that helps metabolize medicine and food and everything (CYP450) that helps metabolize both drugs.
When you combine the two, the metabolism of Descovy may be increased - this is something you will need to bring up with you GI and the provider prescribing PrEP.
This is similar to how you can’t take SSRIs (lexapro, etc), birth control or other similar medicine with grapefruit! It’s a cool mechanism but not cool for your liver.
Doesn’t mean a hard “No” neccessarily, just may need more monitoring or dose changes!
Small Molecules (S1P Inhibitors Like Zeposia, Rinqoq and Friends)


Corticosteroids (Prednisone, Methylprednisolone)
Corticosteroids really aren’t supposed to be used long term, so this shouldn’t be that big of an issue, but if you are on long term steroids, you may need to make sure your PCP or provider that monitors your PrEP is aware of everything you take so they can keep an extra eye on your lab work.
Coadministration of descovy with prednisone (taking it at the same time) can reduce your renal function
Taking both at the same time will reduce both of their therapeutic effect and reduce the serum concentration of both, (as methylprednisolone is a CYP3A4 enzyme inducer and descovy is metabolized by the CYP3A4 enzyme.
This is the same side effect as some of the other medications like thiopurines, combining steroids and descovy may lead to increased serum concentrations of the medicine, possibly decreasing the effectiveness.

Antibiotics in IBD
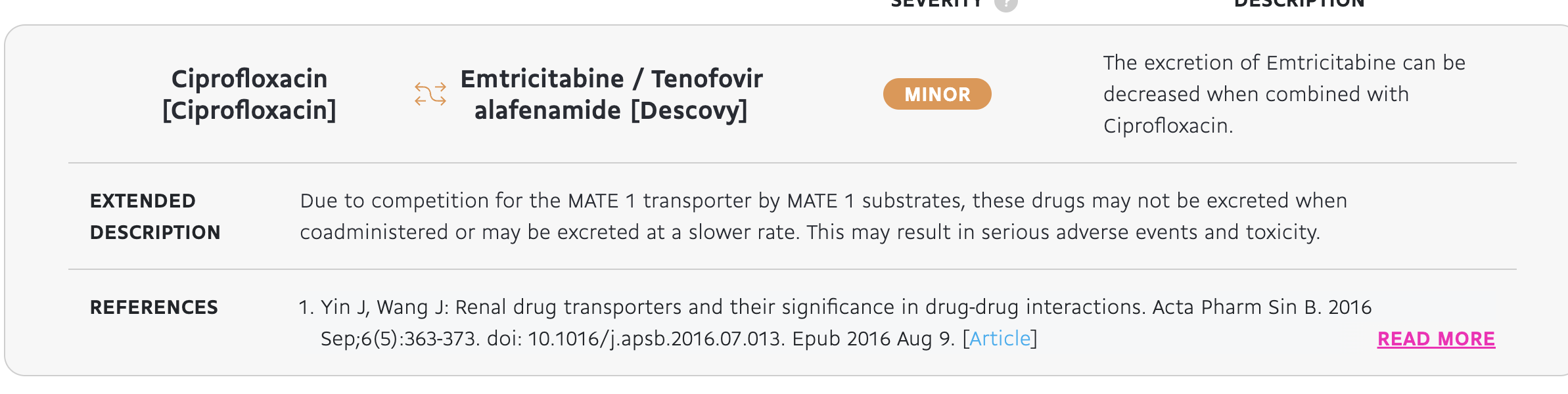
Antibiotics commonly prescribed in IBD (lets hear it for everyone on that #CiproFlagyl combo) may have some potential interactions with PrEP.
These interactions are not extremely harmful (as in, your liver isn’t going to explode and your kidneys aren’t going to melt if you take antibiotics and PrEP), and are mostly related to how the medications are absorbed.
When taking Cipro, the excretion of one part of Descovy (tenofovir) may be decreased at a slower rate because of both drugs competing for the same transporter to use in the kidney (that silly MATE1 is so popular)
At the same time, the serum concentration (the concentration of it in your blood) of Tenofovir can be increased when it is combined with Ciprofloxacin because they are both competing for that sweet, sweet kidney time. (popular organ apparently)
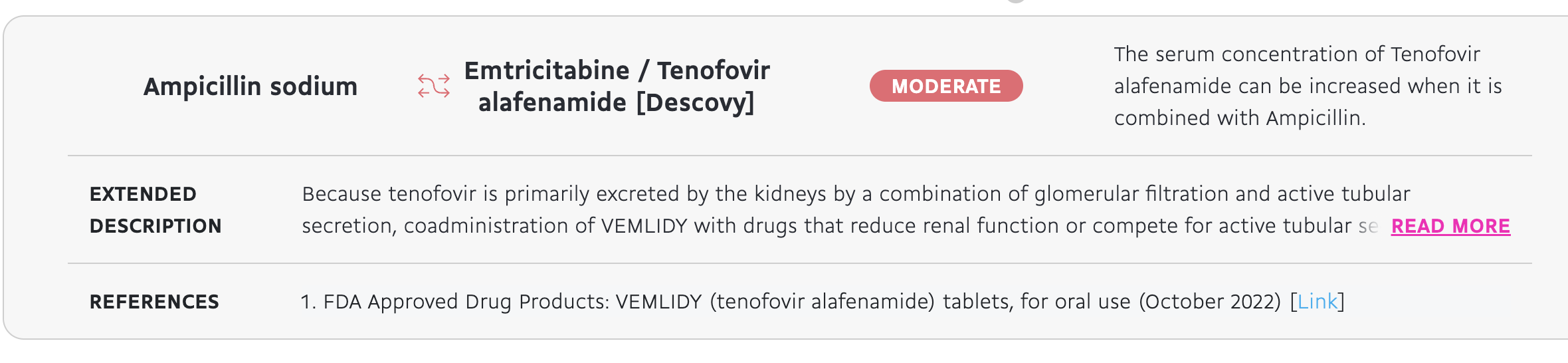
If you guessed the kidneys with ampicillin, you would also be correct.
This is because Tenofovir is processed through the kidneys, so taking other meds processed through the kidneys like Ampicillin can put more strain there.


From DrugBank, a database used for drug discovery, clinical research and academic research.
Knox C, Wilson M, Klinger CM, et al. DrugBank 6.0: the DrugBank Knowledgebase for 2024. Nucleic Acids Res. 2024 Jan 5;52(D1):D1265-D1275. doi: 10.1093/nar/gkad976.
Law V, Knox C, Djoumbou Y, Jewison T, Guo AC, Liu Y, Maciejewski A, Arndt D, Wilson M, Neveu V, Tang A, Gabriel G, Ly C, Adamjee S, Dame ZT, Han B, Zhou Y, Wishart DS. DrugBank 4.0: shedding new light on drug metabolism. Nucleic Acids Res. 2014 Jan 1;42(1):D1091-7.
Wishart DS, Feunang YD, Guo AC, Lo EJ, Marcu A, Grant JR, Sajed T, Johnson D, Li C, Sayeeda Z, Assempour N, Iynkkaran I, Liu Y, Maciejewski A, Gale N, Wilson A, Chin L, Cummings R, Le D, Pon A, Knox C, Wilson M. DrugBank 5.0: a major update to the DrugBank database for 2018. Nucleic Acids Res. 2017 Nov 8. doi: 10.1093/nar/gkx1037.
Wishart DS, Knox C, Guo AC, Cheng D, Shrivastava S, Tzur D, Gautam B, Hassanali M. DrugBank: a knowledgebase for drugs, drug actions and drug targets. Nucleic Acids Res. 2008 Jan;36(Database issue):D901-6.
Knox C, Law V, Jewison T, Liu P, Ly S, Frolkis A, Pon A, Banco K, Mak C, Neveu V, Djoumbou Y, Eisner R, Guo AC, Wishart DS. DrugBank 3.0: a comprehensive resource for 'omics' research on drugs. Nucleic Acids Res. 2011 Jan;39(Database issue):D1035-41.